Contents
Physical Activity Assessment Domain
Introduction- What is physical activity?
- Energy expenditure
- Movement
- Posture
- Volume, intensity, duration, frequency
- Physical behaviour type
- Contextual information: Domain, spatial settings and social contexts
- Sedentary behaviour
- Physical activity guidelines
- Physical activity variation
- Inventory and taxonomy of pattern metrics
- Introduction to objective methods
- Pedometers
- Accelerometers
- Heart rate monitors
- Combined heart rate and motion sensors
- Direct observation
- Doubly labelled water
- GPS and other GNSS receivers
- Multi sensor monitors
- Harmonisation of physical activity data
- Case study: Physical activity during pregnancy and anthropometry of the offspring
- Comparison of three harmonisation methods using validation data
- Network harmonisation of physical activity data using validation data
- Physical Activity Assessment Video Resources
- Getting participants started with the Axivity Monitor
- Wearing the Axivity Monitor
- Getting participants started with the ActiGraph Monitor
- Getting participants started with the Actiheart Monitor
- Wearing the ActiGraph monitor
- Step Test Procedure
Combined heart rate and motion sensors
Combined heart rate and motion (HR+M) sensors measure two phenomena:
- Heart rate, a physiological response to physical activity
- Acceleration due to body movement, a biomechanical variable
The measurement errors from the two methods are not positively correlated; they may even (ideally) be negatively correlated (Brage et al, 2004). At lower levels of intensity, heart rate is less accurate at estimating energy expenditure; this is the level that accelerometers generally have low error. Conversely, activities performed at moderate-to-vigorous intensity, especially biomechanically diverse activities, are assessed with great uncertainty with accelerometry but are measured well with heart rate monitoring. Activities not measured well by waist-mounted accelerometers such as cycling, walking on incline, carrying weights and activities involving predominantly upper-body work are also captured by heart rate monitoring (Brage et al., 2005a; Strath et al., 2005).
The HR+M method provides detailed data on frequency, intensity and duration of physical activity. Aside from doubly labelled water and indirect calorimetry, it is one of the most accurate methods for estimating physical activity energy expenditure over extended durations (Assah et al., 2011; Brage et al., 2015; Villars et al., 2012; Zakeri et al., 2008). Combined HR+M sensors do not provide information on the qualitative dimensions of physical activity, such as context or type. The dimensions of physical activity assessed by combined heart rate and movement sensors are described in Table P.3.13.
Table P.3.13 The physical activity dimensions which can be assessed by combined HR+M sensors.
| Dimension | Possible to assess? |
|---|---|
| Duration | ✔ |
| Intensity | ✔ |
| Frequency | ✔ |
| Volume | ✔ |
| Total physical activity energy expenditure | ✔ |
| Type | ✔ |
| Timing of bouts of activity (i.e. pattern of activity) | ✔ |
| Domain | |
| Contextual information (e.g. location) | |
| Posture | ✔ |
| Sedentary behaviour | ✔ |
Heart rate and accelerometer data can be captured simultaneously using two separate devices (Strath et al., 2001) or combination monitors; however the principles of combined sensing modeling can usually be applied regardless of the capturing device(s) used. The first single-piece combined HR+M sensor was reported in 2000 but this device was never available commercially (Rennie et al., 2000). More sophisticated devices are capable of monitoring heart rate using digitalised electrocardiography (ECG) signal and simultaneously measure motion by an integrated accelerometer.
The first commercially available single-piece combined HR+M sensor was the Actiheart, a light-weight water-proof sensor designed to clip onto two standard ECG electrodes, capable of capturing uniaxial acceleration and average heart rate in short epochs over 11 days (Brage et al., 2005a). Intra- and inter-instrument reliability and validity of the heart rate and motion sensor during electronically simulated heart rate, mechanical shaking, and specific activities conducted during laboratory conditions have been assessed (Brage et al., 2005a; Crouter et al., 2008; Thompson et al., 2006), and it has also been validated against doubly labelled water (DLW) (Assah et al., 2011; Brage et al., 2015). Other combined sensors include the chest belt-based ActiReg, Ickal, Wahoo Fitness TICKR, Garmin HRM-Pro and Actitrainer (Hustvedt et al., 2004; Ojiambo et al., 2012), and wrist-worn devices with accelerometer and optical heart rate sensors such as Apple Watch, Samsung Galaxy Watch, Garmin Forerunner, Honor Magic watch, Fitbit Charge HR (Stahl et al., 2016).
Combined HR+M sensor placement
- Chest-worn ECG-electrode based devices (e.g. Actiheart) are positioned on at least two ECG electrodes, positioned reasonably horizontally (e.g. at V5) but without the monitor pulling the points of skin contact; this could add noise to the heart rate readings and also cause discomfort.
- Multiple-piece devices with chest belt-based heart rate monitoring (e.g. ActiReg) are sensitive to positioning of the motion sensors only.
- Single-piece chest belt-based devices (e.g., Actitrainer, Wahoo, Garmin HRM-Pro) may be bulkier but are almost impossible to position wrongly; the strap goes around the chest with the belt-electrodes making close contact with the skin.
- Wrist-worn devices (e.g. Fitbit Charge HR, Garmin VivoSmart HR+) are also easy to place; they are worn just like a wrist watch. Close skin contact is also essential for these to optimise light transmission and detection by the photodiode and minimise light from external sources.
- Misalignment of uniaxial accelerometers may result in an altered movement signal if the acceleration along the alternative axis is different (Brage et al., 2005a).
- Placement of the monitor on the torso above or below the apex of the sternum has minimal effect on registered movement and estimates of energy expenditure (Brage et al., 2005b).
- Placement of the monitor below the sternum (see Figure P.3.10) may be marginally preferable to reduce noise levels of heart-rate data (Brage et al., 2005b) and is usually preferred by the volunteer.
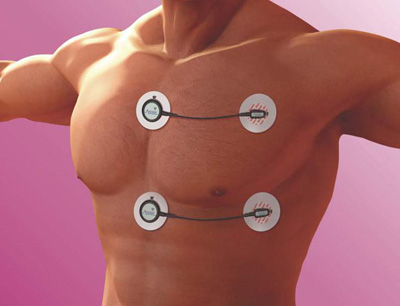

Figure P.3.10 Top panel: Upper and lower positions for ECG electrode-based combined sensor attachment. The accelerometer in this device is placed in the larger round clip orthogonally to the wire axis, thus here orientated to measure accelerations along the longitudinal axis of the body. Bottom panel: Combined heart rate and movement sensor on wrist.
Calibration
The relationship between heart rate and physical activity energy expenditure is different between individuals as explained in the heart rate monitoring section. Individual calibration will therefore also improve precision for combined sensing estimates. Resources will be required for individual calibration which will vary according to the method of calibration. One study investigated the following range of calibration techniques, shown below with decreasing level of complexity:
- Wide-range graded ergometer test with EE measurement
- Wide-range graded ergometer test with estimated EE profile
- Moderate-range graded step test with EE measurement
- Moderate-range graded step test with estimated EE profile
- Low-range walk test with EE measurement
- Low-range walk test with estimated EE profile
- No dynamic calibration (using only resting heart rate, age, sex, etc)
Simple calibration techniques (walk and step test) were shown to achieve acceptable levels of accuracy for the combined technique to be considered as an objective measure in population studies (Brage et al., 2007).
A flexible but consistent approach to calibration has been suggested which spans individual calibration over a range of intensities, to the use of non-dynamic calibration accounting for parameters known to affect the heart rate – energy expenditure relationship, such as age, sex or sleeping heart rate (Andrews, 1971; Brage et al., 2007; Rennie et al., 2001; Strath et al., 2005). There is a trade-off between the validity and feasibility of different individual calibration methods as shown in Figure P.3.11.

Figure P.3.11 Trade-off between validity and feasibility of calibration procedures. Adapted from: Brage et al., 2007.
GXT: graded exercise test; XT: exercise test.
The software of some combined sensor platforms incorporates facilities for conducting exercise tests that permits individual calibration of the HR-EE relationship. Individual calibration may, however, be performed with any device which measures heart rate using graded exercise test protocols (e.g. step frequency audio prompt available from www.mrc-epid.cam.ac.uk). All that is required is that the raw heart rate data are exported and analysed in standard statistical packages with appropriate programming.
- Combined heart rate and movement sensing is suitable for observational as well as intervention studies.
- Although combined sensors are still relatively expensive, they have been used in large population based studies (> 10,000 participants) suggesting that they are a feasible option in epidemiological research. Newer devices, particularly wrist monitors, are cheaper and therefore a more feasible option in terms of cost, and as with most wearable technology prices in general are likely to fall.
- Validation studies suggest that combined heart rate and movement sensors have great utility as measures of physical activity behaviour in free-living adults and children; depending on feasibility aspects of individual monitor types.
There are three main approaches for deriving estimates of physical activity from combined heart rate and acceleration data:
- Multiple linear regression equations on ‘representative data’
- Conditional modeling with a priori biological concepts
- Complex non-linear modeling, e.g. splines
Multiple regression equations
The first study to demonstrate the utility of combined HR+M sensing to improve estimates of physical activity used multiple linear regression (Avons et al., 1988). Further studies showed that using regression analyses to predict energy expenditure from motion sensors combined with heart rate increased explained variance of criterion energy expenditure compared to use of heart rate alone (Haskell et al., 1993; Luke et al., 1997) these earlier studies did not consider individual calibration. Moon et al. (1996) tested 13 linear and non-linear functions, but found that the use of movement sensing to assign heart rate to either an ‘active’ curve, or ‘inactive’ curve resulted in the lowest prediction error (~3.3%). This type of conditional modelling is discussed further below.
Conditional modelling
Conditional modelling involves different treatment of the same raw value depending upon a set of criteria; “If [condition], then do one thing, if not [condition], then do another thing with the same raw value” (see Figure P.3.12). This commonly results in the raw value being entered into one of a selection of regression equations to predict energy expenditure. The above example from work Moon et al is a form of condition modelling.
Rennie et al. (2000) also used individually established heart rate – energy expenditure relationships; one ‘sedentary’ and one ‘active’. The choice of which relationship to use was made based upon a movement count threshold, a method that resulted in high validity in a small calorimetry study. Strath et al. (2001) used two individually established heart rate – energy expenditure relationships (one ‘arm-only’ and one ‘leg/whole-body’), depending on the ratio between leg and wrist accelerometers. This resulted in greater precision of the physical activity energy expenditure estimation.
Branched equation modelling was examined in a study that used the combination of heart rate monitoring and accelerometry against whole-body calorimetry (Brage et al., 2004). Physical activity energy expenditure was estimated with four different weightings for the accelerometer data and heart rate data depending on the intensity of the activity (Brage et al., 2004). That is, in low levels of movement and heart rate the accelerometry data is mainly relied upon, and at very high intensities only heart rate data are lied upon, with two interim weightings in between. Low to moderate activities performed by adults in a laboratory setting were well-captured by branched equation modelling of the two sources of information (Thompson et al., 2006). Another evaluation of branched equation modelling validated against indirect calorimetry during a wide range of activities in a laboratory setting also reported that this particular technique produces valid estimates (Crouter et al., 2008). Free-living evaluations against DLW in Europe and Africa suggest that the method is valid for predicting PAEE (Assah et al., 2011; Brage et al., 2015; Ojiambo et al, 2012).
")
Figure P.3.12 Branched equation modelling is a decision tree for determining the weighting in the weighted average between physical activity intensity determined by heart rate and physical activity intensity determined by accelerometer; the heart rate estimate is weighed the heaviest when both heart rate and movement levels are high, where the accelerometer estimate has greatest weight when both are low. Adapted from: Brage et al., 2004.
Alternative modelling techniques have also been investigated, such as the arm-leg model that accounts for involvement of major muscle groups or only upper limb movement (Strath et al., 2005). Other methods include multivariate adaptive regression splines (MARS) which use multiple segments of polynomial functions that take both local time point inputs and features derived from the time-series data around those local time points (Zakeri et al., 2008).
Irrespective of modelling technique, combined sensing has been shown to accurately reflect physical activity energy expenditure estimation at both a group and individual level.
Identification of non-wear time
Non-wearing time segments in non-labelled activity records from free-living are more easily determined from physiological signals than when using an accelerometer alone, since heart rate can only assume a set range of values from sleeping heart rate to maximal heart rate, whereas “no motion” looks the same in accelerometer measurements, regardless being worn or not. However, attention must be given to handling measurement noise in long-term combined sensing recordings obtained during free-living, a phenomenon which is more common in physiological signals such as heart rate (Stegle et al., 2008). Even so, uncertainty of the signals can be quantified which may then be used to make inferences on wear/non-wear (Brage et al., 2015).
An overview of the characteristics of combined HR+M sensors is outlined in Table P.3.14.
Strengths
Most of the advantages of accelerometry and heart rate monitoring alone are also advantages of combined heart rate and motion measurement:
- Provides an objective measure of physical activity
- Provides an accurate estimate of energy expenditure during physical activity
- Combined measurement has been shown to be reliable and valid at both individual and group level
- Gives a detailed description of activity patterns
- Combined HR+M devices have storage capacity of at least 7 days
- Able to detect change in activity
- Unlikely to induce a large change in behaviour
- Single-piece devices involve a reasonably low individual burden
- Suitable for use in the young and old
- Easy and quick data collection
- Non wearing time easily identified
- Waterproof
- Reasonably low level individual calibration can yield accuracy suitable for epidemiological studies
- Using the combined approach means that many of the drawbacks when the methods are used in isolation are overcome
Limitations
- Some combined HR+M devices are still prohibitively expensive
- Measurement noise can be present in the heart rate data
- The data produced from either combined devices or the two instruments used simultaneously are somewhat complex and requires careful interpretation and guidance (or provision of software) from those experienced in the method. This is particularly true for dealing with measurement noise in HR recordings
- Combining a heart rate monitor with a separate accelerometer imposes an additional individual burden and potential time synchronisation issues
- Compliance may be an issue in some populations especially adolescents
- If using electrodes, individuals may experience an adverse skin reaction to these
Table P.3.14 Characteristics of combined HR+M sensors.
| Consideration | Comment |
|---|---|
| Number of participants | Small to large |
| Relative cost | Moderate to high |
| Participant burden | High with individual calibration |
| Researcher burden of data collection | High with individual calibration |
| Researcher burden of data analysis | Moderate to High |
| Risk of reactivity bias | Yes |
| Risk of recall bias | No |
| Risk of social desirability bias | No |
| Risk of observer bias | No |
| Participant literacy required | No |
| Cognitively demanding | No |
Considerations relating to the use of combined HR+M sensors for assessing physical activity are summarised by population in Table P.3.15.
Combined monitoring of heart rate and movement have been undertaken in in Europe, the Americas, the Arctic, Africa, and Asia, and across the age range of young children to older adults (Assah et al., 2011; Christensen et al., 2012; Collings et al., 2014; Cooper et al., 2015; Dahl-Petersen et al., 2013; Eston et al., 1998; Lindsay et al., 2019; Luke et al., 1997; Rennie et al., 2000; Strath et al., 2001; Strath et al., 2002; Treuth et al., 1998; Vaisto et al., 2014).
Table P.3.15 Physical activity assessment by combined HR+M sensors in different populations.
| Population | Comment |
|---|---|
| Pregnancy | Depending on term, may need to consider placement of monitors to avoid discomfort. Skin can also be more sensitive during pregnancy which could increase chances of irritation. |
| Infancy and lactation | Not suitable. |
| Toddlers and young children | May have difficulty wearing electrodes and chest strap both in terms of having more sensitive skin but also the size of straps and belts of the monitors themselves. There are also small pieces which could be swallowed. Child curiosity could lead to fiddling which interferes with heart rate signal. |
| Adolescents | Skin sensitivity may lead to irritation. |
| Adults | |
| Older Adults | Safety may be a concern when conducting exercise testing for individual calibration. Self-paced protocols may be viable alternatives. Dexterity may be an issue when changing electrodes/placing device. |
| Ethnic groups | |
| Other | In obese individuals it may be more difficult to get a good heart rate signal due to adiposity acting as a signal dampener. |
- Electrodes needs changing during free-living – approximately every second day.
- Individuals should be confident and competent at placing the device, i.e. have sufficient explanation and written instructions provided.
- It may be necessary to involve a third party (e.g. carer or parent) to help with changing electrodes and/or placement of the device.
- Skin irritations from electrodes are more common during warmer weather due to increased heat and sweat. Extensive electrode testing for most useful type in specific contexts advised.
- Chest belt attachment may a good alternative for ECG systems but can also be uncomfortable, particularly for males.
- For wrist-based devices, close skin contact is essential. Other ways to limit external light noise is by covering the device with dark clothes.
The following resources are usually required in addition to trained personnel:
- Combined HR+M device(s) in the form of either:
- Separate HR and movement sensor devices
- An integrated single-piece HR+M device
- Interface (e.g. USB)
- Software (for initialisation/download/analysis)
- Charger
- Additional ECG pads to replace as required (for ECG-based systems)
A list of specific combined heart rate and movement instruments is being developed for this section. In the meantime, please refer to the overall instrument library page by clicking here to open in a new page.
- Anastasopoulou P, Tubic M, Schmidt S, Neumann R, Woll A, Härtel S. Validation and comparison of two methods to assess human energy expenditure during free-living activities. PLOS ONE. 2013;9:e90606
- Andrews RB. Net heart rate as a substitute for respiratory calorimetry. The American Journal of Clinical Nutrition. 1971;24:1139-47
- Assah FK, Ekelund U, Brage S, Wright A, Mbanya JC, Wareham NJ. Accuracy and validity of a combined heart rate and motion sensor for the measurement of free-living physical activity energy expenditure in adults in Cameroon. International Journal of Epidemiology. 2010;40:112-20
- Avons P, Garthwaite P, Davies HL, Murgatroyd PR, James WP. Approaches to estimating physical activity in the community: calorimetric validation of actometers and heart rate monitoring. European Journal of Clinical Nutrition. 1988;42:185-96
- Berntsen S, Hageberg R, Aandstad A, Mowinckel P, Anderssen SA, Carlsen KH, Andersen LB. Validity of physical activity monitors in adults participating in free-living activities. British Journal of Sports Medicine. 2008;44:657-64
- Brage S, Brage N, Franks PW, Ekelund U, Wong MY, Andersen LB, Froberg K, Wareham NJ. Branched equation modeling of simultaneous accelerometry and heart rate monitoring improves estimate of directly measured physical activity energy expenditure. Journal of Applied Physiology (Bethesda, Md.:1985). 2003;96:343-51
- Brage S, Brage N, Franks PW, Ekelund U, Wareham NJ. Reliability and validity of the combined heart rate and movement sensor Actiheart. European Journal of Clinical Nutrition. 2005a;59:561-70
- Brage S, Brage N, Ekelund U, Luan J, Franks PW, Froberg K, Wareham NJ. Effect of combined movement and heart rate monitor placement on physical activity estimates during treadmill locomotion and free-living. European Journal of Applied Physiology. 2005b;96:517-24
- Brage S, Ekelund U, Brage N, Hennings MA, Froberg K, Franks PW, Wareham NJ. Hierarchy of individual calibration levels for heart rate and accelerometry to measure physical activity. Journal of Applied Physiology (Bethesda, Md.:1985). 2007;103:682-92
- Brage S, Westgate K, Franks PW, Stegle O, Wright A, Ekelund U, Wareham NJ. Estimation of Free-Living Energy Expenditure by Heart Rate and Movement Sensing: A Doubly-Labelled Water Study. PLOS ONE. 2015;10:e0137206
- Christensen DL, Faurholt-Jepsen D, Boit MK, Mwaniki DL, Kilonzo B, Tetens I, Kiplamai FK, Cheruiyot SC, Friis H, Borch-Johnsen K, et al. Cardiorespiratory fitness and physical activity in Luo, Kamba, and Maasai of rural Kenya. American Journal of Human Biology : the official journal of the Human Biology Council. 2012;24:723-9
- Collings PJ, Wijndaele K, Corder K, Westgate K, Ridgway CL, Dunn V, Goodyer I, Ekelund U, Brage S. Levels and patterns of objectively-measured physical activity volume and intensity distribution in UK adolescents: the ROOTS study. The International Journal of Behavioral Nutrition and Physical Activity. 2013;11:23
- Cooper AJ, Simmons RK, Kuh D, Brage S, Cooper R, NSHD scientific and data collection team. Physical activity, sedentary time and physical capability in early old age: British Birth Cohort Study. PLOS ONE. 2014;10:e0126465
- Corder K, Brage S, Wareham NJ, Ekelund U. Comparison of PAEE from combined and separate heart rate and movement models in children. Medicine and Science in Sports and Exercise. 2005;37:1761-7
- Crouter SE, Churilla JR, Bassett DR. Accuracy of the Actiheart for the assessment of energy expenditure in adults. European Journal of Clinical Nutrition. 2007;62:704-11
- Dahl-Petersen IK, Bjerregaard P, Brage S, Jørgensen ME. Physical activity energy expenditure is associated with 2-h insulin independently of obesity among Inuit in Greenland. Diabetes Research and Clinical Practice. 2013;102:242-9
- Eston RG, Rowlands AV, Ingledew DK. Validity of heart rate, pedometry, and accelerometry for predicting the energy cost of children's activities. Journal of Applied Physiology (Bethesda, Md.:1985). 1998;84:362-71
- Hustvedt BE, Christophersen A, Johnsen LR, Tomten H, McNeill G, Haggarty P, Løvø A. Description and validation of the ActiReg: a novel instrument to measure physical activity and energy expenditure. The British Journal of Nutrition. 2004;92:1001-8
- Haskell WL, Yee MC, Evans A, Irby PJ. Simultaneous measurement of heart rate and body motion to quantitate physical activity. Medicine and Science in Sports and Exercise. 1993;25:109-15
- Lindsay T, Westgate K, Wijndaele K, Hollidge S, Kerrison N, Forouhi N, Griffin S, Wareham N, Brage S. Descriptive epidemiology of physical activity energy expenditure in UK adults (The Fenland study). The International Journal of Behavioral Nutrition and Physical Activity. 2019;16:126
- Patrik Johansson H, Rossander-Hulthén L, Slinde F, Ekblom B. Accelerometry combined with heart rate telemetry in the assessment of total energy expenditure. The British Journal of Nutrition. 2006;95:631-9
- Luke A, Maki KC, Barkey N, Cooper R, McGee D. Simultaneous monitoring of heart rate and motion to assess energy expenditure. Medicine and Science in Sports and Exercise. 1997;29:144-8
- Moon JK, Butte NF. Combined heart rate and activity improve estimates of oxygen consumption and carbon dioxide production rates. Journal of Applied Physiology (Bethesda, Md.:1985). 1996;81:1754-61
- Ojiambo R, Konstabel K, Veidebaum T, Reilly J, Verbestel V, Huybrechts I, Sioen I, Casajús JA, Moreno LA, Vicente-Rodriguez G, et al. Validity of hip-mounted uniaxial accelerometry with heart-rate monitoring vs. triaxial accelerometry in the assessment of free-living energy expenditure in young children: the IDEFICS Validation Study. Journal of Applied Physiology (Bethesda, Md.:1985). 2012;113:1530-6
- Rennie KL, Hennings SJ, Mitchell J, Wareham NJ. Estimating energy expenditure by heart-rate monitoring without individual calibration. Medicine and Science in Sports and Exercise. 2001;33:939-45
- Rennie K, Rowsell T, Jebb SA, Holburn D, Wareham NJ. A combined heart rate and movement sensor: proof of concept and preliminary testing study. European Journal of Clinical Nutrition. 2000;54:409-14
- Stahl SE, An HS, Dinkel DM, Noble JM, Lee JM. How accurate are the wrist-based heart rate monitors during walking and running activities? Are they accurate enough? BMJ Open Sport & Exercise Medicine. 2016;2:e000106
- Stegle O, Fallert SV, MacKay DJ, Brage S. Gaussian process robust regression for noisy heart rate data. IEEE Transactions on Bio-medical Engineering. 2008;55:2143-51
- Strath SJ, Bassett DR, Swartz AM, Thompson DL. Simultaneous heart rate-motion sensor technique to estimate energy expenditure. Medicine and Science in Sports and Exercise. 2001;33:2118-23
- Strath SJ, Bassett DR, Thompson DL, Swartz AM. Validity of the simultaneous heart rate-motion sensor technique for measuring energy expenditure. Medicine and Science in Sports and Exercise. 2002;34:888-94
- Strath SJ, Brage S, Ekelund U. Integration of physiological and accelerometer data to improve physical activity assessment. Medicine and Science in Sports and Exercise. 2005;37:S563-71
- Thompson D, Batterham AM, Bock S, Robson C, Stokes K. Assessment of low-to-moderate intensity physical activity thermogenesis in young adults using synchronized heart rate and accelerometry with branched-equation modeling. The Journal of Nutrition. 2006;136:1037-42
- Treuth MS, Adolph AL, Butte NF. Energy expenditure in children predicted from heart rate and activity calibrated against respiration calorimetry. The American Journal of Physiology. 1998;275:E12-8
- Väistö J, Eloranta AM, Viitasalo A, Tompuri T, Lintu N, Karjalainen P, Lampinen EK, Ågren J, Laaksonen DE, Lakka HM, et al. Physical activity and sedentary behaviour in relation to cardiometabolic risk in children: cross-sectional findings from the Physical Activity and Nutrition in Children (PANIC) Study. The International Journal of Behavioral Nutrition and Physical Activity. 2013;11:55
- Villars C, Bergouignan A, Dugas J, Antoun E, Schoeller DA, Roth H, Maingon AC, Lefai E, Blanc S, Simon C, et al. Validity of combining heart rate and uniaxial acceleration to measure free-living physical activity energy expenditure in young men. Journal of Applied Physiology (Bethesda, Md.:1985). 2012;113:1763-71
- Zakeri I, Adolph AL, Puyau MR, Vohra FA, Butte NF. Application of cross-sectional time series modeling for the prediction of energy expenditure from heart rate and accelerometry. Journal of Applied Physiology (Bethesda, Md.:1985). 2008;104:1665-73

- The Toolkit
- About
- What's new
- Other resources
- Toolkit Team
- Contact
- Links to other toolkits
- Nutritools
- NCI/NIH Dietary Assessment Primer
- © 2026 MRC Epidemiology Unit
- Privacy policy and cookies
- Terms of Use